
64 6.6 Human Responses to High Altitude
Created by: CK-12/Adapted by Christine Miller

High and Hypoxic
This mountain scene of Machu Picchu in the Peruvian Andes is a sight to behold. Lurking behind the beauty of this and some other mountain ranges, however, is a potentially deadly threat to the human organism: high-altitude hypoxia. Hypoxia is literally a lack of oxygen. It occurs to varying degrees at altitudes higher than about 2,500 metres above sea level. Yet despite the high altitude of the location shown in Figure 6.6.1, it is very evident that humans have been thriving in this environment for long periods of time; in fact, Machu Picchu was most likely built in the mid 1400s. Modern day peoples live in high altitude locations all over earth where hypoxia may occur, including the Himalaya Mountains in Asia, the Ethiopian Highlands in Africa, and the Rocky Mountains in North America.
Why Hypoxia Occurs at High Altitudes
Although the percentage of oxygen in the atmosphere is the same at high altitudes as it is at sea level, the atmosphere is less dense at high altitudes. This means that the molecules of oxygen (and other gases) in the air are more spread out, so a given volume of air contains fewer oxygen molecules. This results in lower air pressure at high altitude. Air pressure decreases exponentially as altitude increases, as shown in the graph below (Figure 6.6.2).
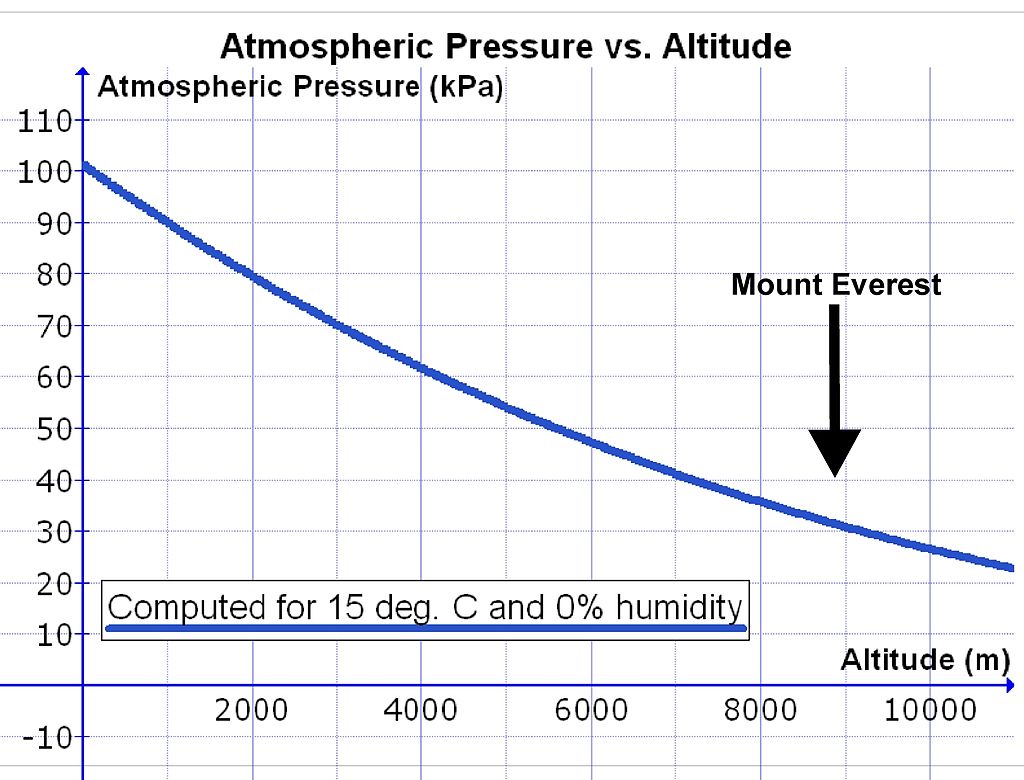
At sea level, air pressure is about 100 kPa. At this air pressure, the air is dense and oxygen passes easily from the air in the lungs through cell membranes into the bloodstream. This is because concentration affects diffusion — the higher the concentration of oxygen in the air we breath, the more it will diffuse into our blood. It is likely we evolved at or near sea level altitudes, so it is not surprising that the human body generally performs best at this altitude. However, as air pressure decreases at high altitudes, it becomes more difficult for adequate oxygen to pass into the bloodstream, and blood levels of oxygen start to fall.
At 2,500 metres above sea level, air pressure is only about 75 per cent of that at sea level, and at five thousand metres, air pressure is only about 50 per cent of the sea level value. The latter altitude is about the altitude of the Mount Everest Base Camp and of the highest permanent human settlement (La Rinconada in Peru, pictured in Figure 6.6.3). Altitudes above 2,500 metres generally require acclimatization or adaptation to prevent illness from hypoxia. Above 7,500 metres, serious symptoms of hypoxia are likely to develop. Altitudes above eight thousand metres are in the “death zone.” This is the zone where hypoxia becomes too great to sustain human life. The summit of Everest, with an altitude of 8,848 metres, is well within the death zone. Mountain climbers can survive there only by taking in extra oxygen from oxygen tanks and not staying at the summit very long.

Physiological Effects of Hypoxia
When a lowlander first goes to an altitude above 2,500 metres, the person’s blood oxygen level starts to fall. The immediate responses of the body to hypoxia are not very efficient, and they place additional stress on the body. The main changes are an increase in the breathing rate (hyperventilation) and an elevation of the heart rate. These rates may be as much as double their normal levels, and they may persist at high levels, even during rest. While these changes increase oxygen intake in the short term, they also place more stress on the body. For example, hyperventilation causes respiratory alkalosis, in which carbon dioxide levels in the blood become too low. The increased heart rate places stress on the cardiovascular system and may be especially dangerous for someone with an underlying heart problem.
The first symptoms of hypoxia the lowlander is likely to notice is becoming tired and out of breath when performing physical tasks. Appetite is also likely to decline, as nonessential body functions are shut down at the expense of maintaining rapid breathing and heart rates. Other symptoms are also likely to develop, such as headache, dizziness, distorted vision, ringing in the ears, difficulty concentrating, insomnia, nausea, and vomiting. These are all symptoms of high altitude sickness.
More serious symptoms may also develop at high altitudes. Fluid collects in the lungs (high altitude pulmonary edema, or HAPE) and in the brain (high altitude cerebral edema, or HACE). HACE may result in permanent brain damage, and both HAPE and HACE can be fatal. The higher the altitude, the greater the likelihood of these serious high altitude disorders occurring, and the greater the risk of death.
Acclimatization to High Altitude

If a lowlander stays at high altitude for several days, the body starts to respond in ways that are less stressful. These responses are the result of acclimatization to high altitude. Additional red blood cells are produced and the tiniest blood vessels, called capillaries, become more numerous in muscle tissues. The lungs also increase slightly in size, as does the right ventricle of the heart, which is the heart chamber that pumps blood to the lungs. All of these changes make the processes of taking in oxygen and transporting it to cells more efficient.
It might occur to you that these changes with acclimatization would improve fitness and performance in athletes, and you would be right. The same changes that help the body cope with high altitude increase fitness and performance at lower altitudes. That’s why athletes often travel to high altitudes to train, and then compete at lower altitudes. Figure 6.6.4 shows Olympic athletes training for long distance running at the Swiss Olympic Training Base in St. Moritz, located in the Swiss Alps.
Full acclimatization to high altitude generally takes several weeks. The higher the altitude, the longer it takes. Even when acclimatization is successful and symptoms of high altitude sickness mostly abate, the lowlander may not be able to attain the same level of physical or mental performance as is possible at lower altitudes. When an altitude acclimatized individual returns to sea level, the changes that occurred at high altitude are no longer needed. The body reverts to the original, pre-high-altitude state in a matter of weeks.
Genetic Adaptations to High Altitude
Well over 100 million people worldwide are estimated to live at altitudes higher than 2,500 metres above sea level. In Table 6.6.1, you can see how these people are distributed in the highest altitude regions around the globe.
Table 6.6.1
Human Populations Residing in High Altitude Regions
| Human Populations Residing in High Altitude Regions | |
| High Altitude Region | Human Population |
| Himalaya-Hindukush-Pamir Ranges, Tibetan Plateau (Asia) | 78,000,000 |
| Andes Mountains (South America) | 35,000,000 |
| Ethiopian Highlands (Africa) | 13,000,000 |
| Rocky Mountains (North America) | 300,000 |
Some Indigenous populations of Tibet, Peru, and Ethiopia have been living above 2,500 metres for hundreds of generations and have evolved genetic adaptations that protect them from high altitude hypoxia. In these populations, natural selection has brought about irreversible, genetically-controlled changes that adapt them to high altitude conditions. As a result, they can live permanently at high altitudes without any, or with only minor, ill effects — even though they are constantly exposed to a level of oxygen that would cause high altitude sickness in most other people. Interestingly, different adaptations evolved in different regions in response to the same stress.
High Altitude Adaptations in Tibetan Highlanders
Highland populations in Tibet, such as the famous Sherpas who serve as Himalaya Mountain guides (see Figure 6.6.5), have lived at high altitudes for only about three thousand years. Their adaptations to high altitude include an increase in the rate of breathing even at rest without alkalosis occurring, and an expansion in the width of the blood vessels (both capillaries and arteries) that carry oxygenated blood to the cells. These changes allow them to carry more oxygen to their muscles and have a higher capacity for exercise at high altitude. Their adaptations to high altitude occurred very rapidly in evolutionary terms and are considered to be the most rapid process of phenotypically observable evolution in humans.

High Altitude Adaptations in Andean Highlanders
Andean highlanders, such as Quechua Native Americans (see Figure 6.6.6), have been living at high altitudes for about 11 thousand years. Their genetic adaptations to high altitude are different than the Tibetan adaptations. They include greater red blood cell volume and increased concentration of hemoglobin, the oxygen-carrying protein that is the main component of red blood cells. These changes allow somewhat higher levels of oxygen to circulate in the blood without increasing the rate of breathing. Compared with other long-term residents at high altitudes, Andean highlanders are the least adapted and most likely to experience high altitude sickness.
 |
 |
 |
| Figure 6.6.6 Quechua Native Americans in the Peruvian Andes. | ||
High Altitude Adaptations in Ethiopian Highlanders

The Ethiopian Highlands (Figure 6.6.7) are high enough to have brought about genetic adaptations in long-term residents. Populations of Ethiopian Highlanders have lived above 2,500 metres for at least five thousand years, and above two thousand metres for as long as 70 thousand years. Many Ethiopian Highlanders today live at altitudes greater than 3,000 metres. However, Ethiopian Highland populations do not appear to have evolved the adaptations that characterize either Tibetan highlanders or Andean highlanders. They do not exhibit the hemoglobin changes or vascular changes of these other highland populations, but they do have greater arterial blood oxygen saturation. Research on Ethiopian adaptations to high altitude has just begun and is still very limited, but they appear to have a unique pattern of adaptation.
6.6 Summary
- At high altitudes, humans face the stress of hypoxia, or a lack of oxygen. Hypoxia occurs at high altitude because there is less oxygen in each breath of air and lower air pressure, which prevents adequate absorption of oxygen from the lungs.
- Initial responses to hypoxia include hyperventilation and elevated heart rate, but these responses are stressful to the body. Continued exposure to high altitude may cause high altitude sickness, with symptoms such as fatigue, shortness of breath, and loss of appetite. At higher altitudes, there is greater risk of serious illness.
- After several days at high altitude, acclimatization starts to occur in someone from a lowland population. More red blood cells and capillaries form and other changes occur. Full acclimatization may take several weeks. Returning to low altitude causes a reversal of the changes to the pre-high-altitude state in a matter of weeks.
- Well over 100 million people live at altitudes higher than 2,500 metres above sea level. Some Indigenous populations of Tibet, Peru, and Ethiopia have been living above 2,500 metres for thousands of years and have evolved genetic adaptations to high altitude hypoxia.
- Different high altitude populations have evolved different adaptations to the same hypoxic stress. Tibetan highlanders, for example, have a faster rate of breathing and wider arteries, whereas Peruvian highlanders have larger red blood cells and a greater concentration of the oxygen-carrying protein hemoglobin.
6.6 Review Questions
- Define hypoxia.
- Why does hypoxia occur at high altitudes?
- Describe the body’s immediate response to hypoxia at high altitude.
-
- What is high altitude sickness, and what are its symptoms?
- What changes occur during acclimatization to high altitude?
- Where would you expect to find populations with genetic adaptations to high altitude?
- Discuss variation in adaptations to high altitude in different high altitude regions.
- Why do you think that adaptations to living at high altitude are different in different regions of the world?
- Using human responses to high altitude as an example, explain the difference between acclimatization and adaptation.
- Why are most humans not well-adapted to living at high altitudes?
- If a person that normally lives at sea level wants to climb a very high mountain, do you think it is better for them to move to higher elevations gradually or more rapidly? Explain your answer.
6.6 Explore More
How People Have Evolved to Live in the Clouds, SciShow, 2019.
The Olympic Altitude Advantage, AsapSCIENCE, 2012.
Alternative Treatment of Altitude Sickness: Manual Medicine | Kelly Riis-Johannessen | TEDxChamonix, TEDx Talks, 2019.
Attributions
Figure 6.6.1
Machu Pichu by Adriana Aceves on Unsplash is used under the Unsplash License (https://unsplash.com/license).
Figure 6.6.2
Altitude_and_air_pressure_&_Everest by Cruithne9 on Wikimedia Commons is used under the CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0/deed.en) license.
Figure 6.6.3
La_Rinconada_Peru by Hildegard Willer on Wikimedia Commons is used under the CC BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0/deed.en) license.
Figure 6.6.4
Swiss_Olympic_training_base by Christof Sonderegger von Photoplus.ch on Wikimedia Commons is used under the CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/4.0/deed.en) license.
Figure 6.6.5
Sherpa guide by McKay Savage on Wikimedia Commons is used under a CC BY 2.0 (https://creativecommons.org/licenses/by/2.0/deed.en) license.
Figure 6.6.6
- Quechua Mother and Child by Thomas Quine on Flickr is used under a CC BY 2.0 (https://creativecommons.org/licenses/by/2.0/) license.
- Tags: Local Community Quechua Indians Grandpa [photo] by Basinatura on Pixabay is used under the Pixabay License (https://pixabay.com/fr/service/license/).
- Tags: Peruvian Traditional Costume Cuzco Andes Peru by SoleneC1 on Pixabay is used under the Pixabay License (https://pixabay.com/fr/service/license/).
Figure 6.6.7
Ethiopian Highlander by Gerald Schömbs on Unsplash is used under the Unsplash License (https://unsplash.com/license).
References
AsapSCIENCE. (2012, July 5). The Olympic altitude advantage. YouTube. https://www.youtube.com/watch?v=wmkO8oWyg8Y&feature=youtu.be
Mayo Clinic Staff. (n.d.). High-altitude pulmonary edema [online article]. MayoClinic.org. https://www.mayoclinic.org/diseases-conditions/pulmonary-edema/multimedia/img-20097483
SciShow. (2019, May 23). How people have evolved to live in the clouds. YouTube. https://www.youtube.com/watch?v=elOn5ZYg5fc&feature=youtu.be
TEDx Talks. (2019, March 27). Alternative treatment of altitude sickness: Manual medicine | Kelly Riis-Johannessen | TEDxChamonix. YouTube. https://www.youtube.com/watch?v=aIOaYh9Bkds&feature=youtu.be
Wikipedia contributors. (2020, April 13). High-altitude cerebral edema. In Wikipedia. https://en.wikipedia.org/w/index.php?title=High-altitude_cerebral_edema&oldid=950658590
A condition in which the body or a region of the body is deprived of adequate oxygen supply at the tissue level.
The negative health effect of high altitude, the mildest form being acute mountain sickness (AMS), caused by rapid exposure to low amounts of oxygen at high elevation. Symptoms may include headaches, vomiting, tiredness, trouble sleeping, and dizziness.
The differential survival and reproduction of individuals due to differences in phenotype. It is a key mechanism of evolution, the change in the heritable traits characteristic of a population over generations.

{kind=link}
{kind=link}
{kind=link}
{kind=link}